All living beings have by nature a "built-in" survival instinct.
There is no single "bad" or unnecessary molecule in the body.
Without LDL-cholesterol, the body will not survive.
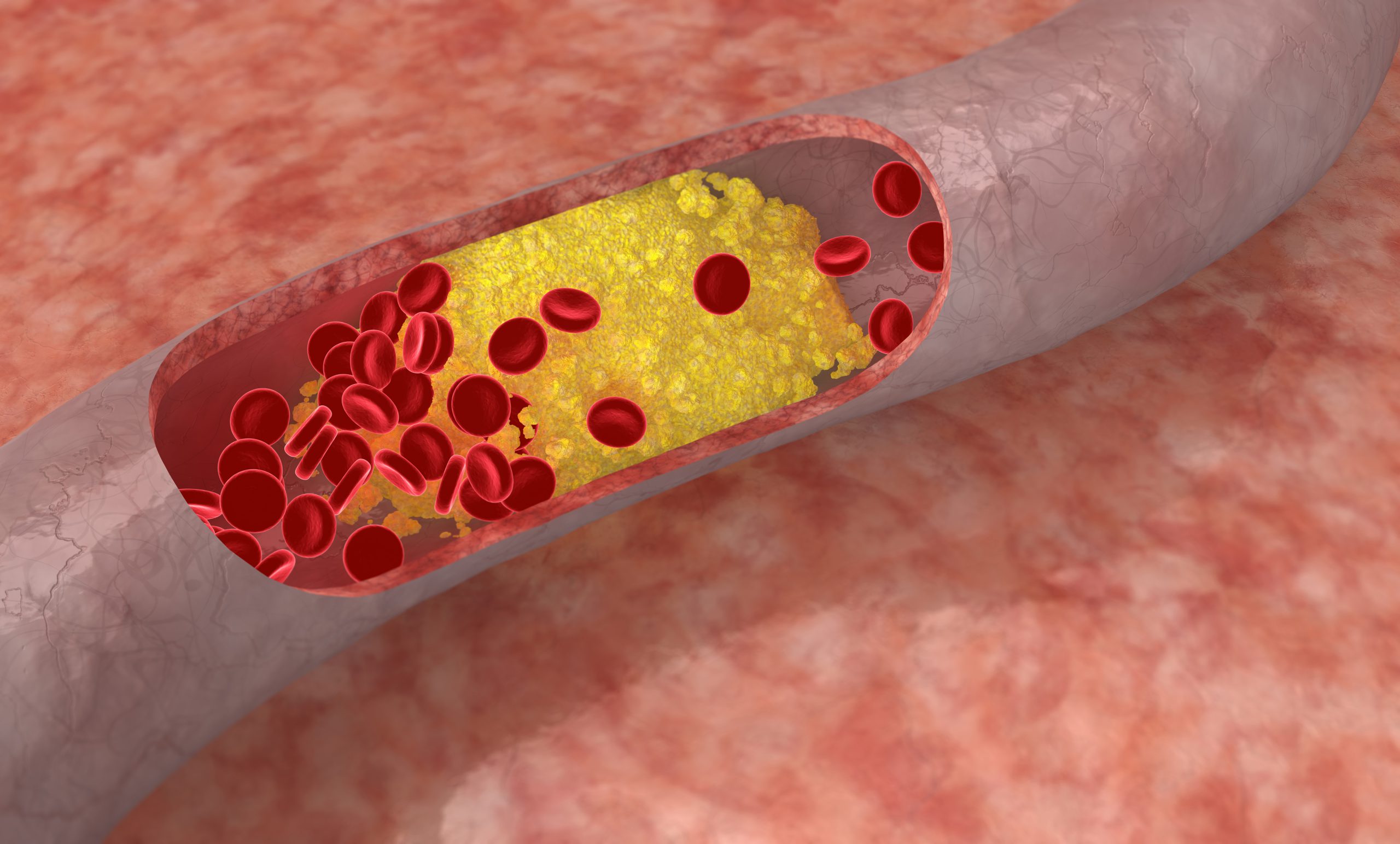
The medical establishment got the public used to the idea that a type of cholesterol called LDL (an abbreviation for “Low Density Lipoprotein”) is “bad”. Anything “bad” in the body gets by nature to be either eliminated or excreted from the body. However, if all the “bad” LDL cholesterol were to be excreted from the body, we would not survive.
What is the LDL cholesterol? It is merely the carrier of fatty acids synthesized in the liver. LDL’s function is to deliver those fatty acids from the liver to its many target sites in the body. Fatty acids are a major vital nutrient, and without the LDL “trucks” carrying them in the blood stream, there would not be a functioning nervous system, no brain and heart function, the skin and hair would dry up and fall and survival hormones, as well as the sex hormones, would cease to be produced. What is referred to by the medical establishment as “good cholesterol” (HDL) is no more than the carriers going in the opposite direction, delivering the old and used cholesterol molecules from the target cells back to the liver for dismantling. Therefore, there is no viable distinction between LDL and HDL in terms of their mare function – i.e. lipid carriers. An excess of HDL (“good”) cholesterol is just as pathological as an excess of LDL. but none of them are the actual pathology. Excess LDL or HDL are mere symptoms of an internal metabolic disturbance, causimg the body to create an excess of those carriers.
Moreover, the amount of LDL molecules in the blood is not the most significant factor when assessing a risk to the heart. What is much more significant for the heart’s health is a right ratio of LDL to HDL, namely 3.5.-3 LDL to 1 HDL. Ideally, LDL should count in the blood around 135 while HDL around 45. But reasonably LDL or HDL higher or lower levels are of less significance to the heart. As long as the said ratio between the two is maintained, reasonable rise in the blood levels of LDL should not be alarming and does not constitute a cardiac risk. As with all else in the body, there should never be an expectation of uniform levels of metabolic markers. Such an unrealistic outlook, prevalent in the medical establishment, is often a cause for misunderstandings and unnecessary medical interventions that might themselves create serious health issues. A reasonable amount of LDL molecules detected in the blood stream is naturally different from person to person according to their age, personal metabolic needs and personal medical history.
Globally
33%of ischemic heart disease cases are attributable to high cholesterol
The prevalence of elevated total cholesterol in Europe is
54%for both sexes
Nearly
29millionadult Americans have total cholesterol levels higher than 240 mg/dL
In the U.S.A
7%of children and adolescents from age 6 to 19 have high total cholesterol.
High levels of LDL in the blood are not a pathology by itself, but a symptom of an internal pathology – usually in the liver, which produces LDL. In the majority of the cases, the liver dysfunction is also related to malabsorption in the gut, resulting in protein and lipid deficiencies. A deficiency in fats consumed or absorbed from the food combined with liver weakness result in a decrease of fatty acids production, which are so vital to the body. To try and compensate for the deficiency in the fatty acids, the liver is driven to produce more and more “fatty acid carriers”, which are the LDL molecules. Therefore, taking pills to forcibly reduce LDL levels does not constitute a solution to any of the root pathologies resulting in excess LDL production. The pills merely inhibit the liver from “doing its job”. The efficient way to solve the problem from its root is to first change the diet to include quality fat and proteins, restore the absorption function of the digestive system and rehabilitate liver function. This treatment of the root causes will also, as a byproduct, reduce excess LDL production levels. Thus the problem of hyperlipidemia will be eliminated from the root without the need to target the LDL with pills laden with detrimental side effects and risks.
One kind of pills usually prescribed by conventional medicine for high levels of LDL are anti-coagulants (also referred to as “blood thinners”). Those pills do not address the underlying pathology of nutrient deficiencies and liver dysfunction. They create an illusion of improvement in the blood contents, much like “cleaning” the house by sweeping the dirt under the carpet. Moreover, with long-term usage, those “blood thinners” eventually weaken the wall of the blood vessels up to creating tears, thereby increasing the danger of internal bleeding. Internal bleeding not only causes blood deficiency (anemia), but also creates blood clots – the very pathology those pills were intended to prevent in the first place. The said blood clots caused by the internal bleeding roam inside the blood vessels till they create a blockage. When such a blockage occurs in major blood vessels leading to the brain or the heart, strokes and heart attacks occur – all due to the prolonged usage of the “blood thinners”.
It should also be noted, that most of pills are synthetic derivatives of aspirin. Originally, aspirin was prepared naturally from the willow tree, but that was switched to a synthetic lab preparation, which damages and weakens the liver and kidneys even further.
The second type of pills commonly prescribed by the allopathic medicine in cases of high blood cholesterol belong to a group called Statins. Statins inhibit the vital action of a major liver enzyme, thereby disrupting producing of LDL. However, this vital enzyme controls many other major functions of the liver too. The idea of blocking a vital and natural metabolic process to treat a symptomatic disorder of the body seems to be an absurd. The proof that blocking this enzyme and inhibiting the liver is not promoting health by any way is the long list of side effects caused by the Statins, listed in the patient’s package insert and proven in many clinical studies.
Over time and with a prolonged usage of Statins, an inflammation of the liver might erupt, eventually causing cirrhosis and even liver cancer. And all of this to reduce the number of fatty acid carriers, which are a mere symptom, and not a root pathology. Moreover, the efficacy of Statins is being reduced with a prolonged usage. Throughout all this time, the patient has starved and depleted the body, causing a dangerous deficiency in essential fatty acids. The result would be a multi-systemic damage far worse than the original problem for which those Statins were prescribed in the first place.

